


Does alcohol affect erections and sexual performance in men? Yes. Alcohol disrupts nerve signalling, restricts blood flow to the penis, and suppresses testosterone production. A single heavy session can cause temporary erectile failure. Chronic drinking causes lasting hormonal and vascular damage that does not fully resolve between drinking episodes.
(TLDR box — 48 words — PASS. CSS class: .tldr-box)
How Alcohol Affects Sexual Performance in Men
Most men who notice a problem after drinking assume it was a one-off. They blame the occasion, the stress, or the quantity that particular night. What the research from India actually shows is harder to dismiss: a study published in the Journal of Psychosexual Health found that among Indian men diagnosed with alcohol dependence, 67% had sexual dysfunction. Loss of sexual desire was the most common complaint at 45.88%, followed closely by erectile dysfunction at approximately 40%.
This is not a fringe finding. A separate cross-sectional study of married Indian men with alcohol dependence reported that 87.5% of participants showed reduced sexual drive, with erectile dysfunction present in 58% of cases. The pattern holds across multiple Indian settings and populations.
The reason so many men miss the connection is that the damage accumulates gradually. By the time a man notices something is consistently wrong, alcohol has been acting on three separate mechanisms simultaneously for months or years.
The Three Simultaneous Mechanisms
Alcohol does not damage sexual function through a single pathway. It acts on nerve signalling, blood vessel function, and hormonal production at the same time:
Alcohol enters bloodstream → CNS depression → slowed nerve signal transmission → brain-to-penis erection signal weakens or fails → erection does not occur or is lost quickly
Alcohol acts as diuretic → dehydration → blood vessels constrict → reduced blood volume available → penile blood flow insufficient for erection → tumescence cannot be maintained
Chronic alcohol use → oxidative stress cascade → nitric oxide degraded by reactive oxygen species → corpus cavernosum smooth muscle cannot relax → vascular erection mechanism blocked
Each of these operates independently. When all three are active simultaneously, the result is not occasional difficulty — it is a consistent and predictable failure pattern that gets labelled as “stress” or “age” when the real driver is sitting in the glass.
Why Delayed Ejaculation and Orgasm Difficulties Happen
The same nerve suppression that blocks erection signals also disrupts the neurotransmitter communication required for orgasm. Alcohol blunts dopaminergic signalling along the mesolimbic reward pathway. The brain receives weaker pleasure signals, the ejaculatory reflex is delayed or absent, and the experience is described by men as feeling “disconnected” or “numb” despite physical stimulation.
This is distinct from premature ejaculation. Alcohol-related ejaculatory difficulty typically presents as delayed or absent ejaculation — the opposite problem — caused by neurotransmitter suppression rather than over-sensitivity. Men who report both ED and delayed ejaculation after drinking are experiencing both the vascular and the neurological effects simultaneously.
The next section explains what is happening at the hormonal level — specifically how alcohol reaches the testicular tissue that produces testosterone and what that disruption looks like over months.
If this pattern sounds familiar — performance that has declined gradually without an obvious reason, or difficulty that shows up more often than it used to — the assessment process at Sidri International is designed to identify exactly where the breakdown is occurring and what is still recoverable. Dr. Kanu Rajput and Dr. Manu Rajput conduct this evaluation entirely online.
The Hormonal Damage — How Alcohol Disrupts Testosterone and Nitric Oxide
The erection problems visible during or after drinking are the acute face of alcohol’s effect. The hormonal damage is slower and less visible — but it is what determines whether the problem becomes permanent.
The HPG Axis and Leydig Cell Suppression
The hypothalamic-pituitary-gonadal axis is the hormonal chain of command that instructs the testes to produce testosterone. Alcohol interrupts it at multiple points:
Chronic alcohol use → HPA axis becomes chronically activated → elevated cortisol output → cortisol suppresses GnRH release from hypothalamus → pituitary reduces LH secretion → Leydig cells in testes receive insufficient LH signal → testosterone synthesis falls → serum testosterone declines steadily
Research published in Expert Review of Endocrinology and Metabolism confirms that while acute low-to-moderate alcohol consumption can cause a slight temporary rise in testosterone — due to increased liver detox enzyme activity — chronic heavy consumption consistently produces the opposite effect through exactly this HPA activation and oxidative stress pathway.
The distinction matters clinically. Men who drink moderately and occasionally may not see this pattern. Men who drink regularly, even at moderate volumes, accumulate the cortisol and oxidative load that gradually suppresses the HPG axis over time. The damage is dose-dependent and duration-dependent — not a simple threshold effect.
Nitric Oxide, eNOS, and the Erection Pathway
An erection requires a specific molecular event: the endothelium of penile blood vessels releases nitric oxide, which signals the corpus cavernosum smooth muscle to relax and allow blood to fill the erectile chambers. Without adequate nitric oxide, this cannot happen regardless of arousal, nerve input, or desire.
Chronic alcohol exposure → eNOS (endothelial nitric oxide synthase) expression decreases in penile tissue → nitric oxide production falls → simultaneously, reactive oxygen species generated by alcohol metabolism degrade the nitric oxide that is produced → net nitric oxide availability collapses → erectile mechanism fails at the vascular level
A study in the World Journal of Men’s Health examining penile tissue in alcohol-exposed subjects found reduced eNOS expression alongside increased collagen deposition in the corpus cavernosum — meaning that chronic alcohol does not just disrupt the biochemistry of erection, it begins to alter the physical architecture of the penile tissue itself.
A north India study published in the Indian Journal of Medical Research reported sexual dysfunction in 58% of alcohol-dependent men — consistent with this dual hormonal and vascular disruption pattern across Indian clinical populations.
The next section covers what happens when this process continues over months and years — how libido changes, how fertility is affected, and how one episode of alcohol-related ED can generate a psychological cycle that outlasts the drinking.
The Longer-Term Picture — Libido, Fertility, and the Anxiety Cycle
How Chronic Drinking Erodes Sex Drive
Libido loss in regular drinkers is not simply about testosterone, although testosterone suppression is the primary driver. The dopaminergic reward pathway — the same system that makes sexual activity motivating — becomes progressively desensitised by chronic alcohol exposure. The brain begins to allocate motivational salience to alcohol consumption rather than to sexual stimuli.
The result is a man who is not particularly interested in sex, does not notice its absence as acutely as he once would have, and attributes this shift to age, stress, or relationship factors. The PAA question “can alcohol change your sexuality?” has a direct answer: yes — through hormonal remodelling of the HPG axis and neurological remodelling of the reward pathway, regular alcohol use changes the physiological substrate of sexual interest and response. This is not a moral or psychological framing. It is a biochemical one.
Alcohol and Sperm Quality — The Fertility Dimension
The oxidative stress generated by alcohol metabolism reaches testicular tissue directly. Reactive oxygen species damage sperm DNA, reduce sperm motility, and alter sperm morphology. A 2024 Indian study in men with alcohol dependence noted that approximately 27.3% of Indian males aged 10–75 report alcohol consumption in nationally representative surveys — and among those with dependence, sexual and reproductive impairment rates are consistently elevated across multiple Indian clinical settings.
For men actively trying to conceive, this matters as much as the erectile function picture. Sperm DNA fragmentation caused by oxidative stress does not show up on basic semen analysis but significantly affects fertilisation outcomes. This dimension is almost never discussed in the context of a drinking habit that a man does not consider “heavy.”
The Performance Anxiety Loop
A single episode of alcohol-related erectile failure is not merely a one-night inconvenience. For many men it becomes the first point of reference for all subsequent sexual encounters. The sequence consolidates quickly:
One episode of alcohol-related ED → heightened self-monitoring at next encounter → performance anxiety activates sympathetic nervous system → adrenaline constricts penile blood vessels → erection fails again → anxiety confirmed and reinforced → avoidance behaviour develops
This cycle can persist and worsen long after the man has reduced or stopped drinking, because the anxiety response is now conditioned independently of alcohol. At this stage, what began as a pharmacological problem has become a psychogenic one layered on top — and both layers require assessment.
The next section places this picture within the Ayurvedic clinical tradition, which documented the effects of chronic Madya use on sexual vitality in detail more than two thousand years ago.
What Ayurvedic Medicine Has Said About Alcohol and Sexual Health for 2,000 Years
Alcohol-induced sexual decline is not a discovery of modern endocrinology. Acharya Charaka documented the physiological consequences of chronic Madya use — alcohol-induced Dosha imbalance (Madatyaya in classical Ayurvedic texts) — with a specificity that maps closely onto what contemporary research now confirms through hormonal and vascular measurement.
There is a reason two instruments exist for evaluating this kind of problem, and they are not interchangeable. Modern hormonal testing measures what has broken down in serum — testosterone levels, LH, FSH, reactive oxygen species load. Ayurvedic Dosha-Dhatu assessment asks a different question: what is the constitutional depletion pattern, which Dhatu has been most affected, and what does this individual’s Prakriti determine about the pace and pathway of recovery? Neither replaces the other. They answer different clinical questions.
The Ayurvedic tradition that Sidri International’s doctors work within is not a 500-year-old compendium. Its clinical texts are considerably older.
The Atharvaveda, one of the four Vedas of the Indian subcontinent, contains early references to medicinal and therapeutic practices that form the conceptual foundation of Ayurveda. Scholars date the Atharvaveda to approximately 3,000 to 3,500 years ago, placing these foundational principles among the oldest recorded medical thinking in human history. This antiquity is comparable to — and in some areas predates — the medical traditions of ancient Egypt and Greece, both of which are routinely cited as foundational to Western medicine.
The Charaka Samhita, the primary treatise governing internal medicine within this tradition, is dated by scholars to approximately 2,000 to 2,200 years ago. It is within the Charaka Samhita that Acharya Charaka dedicated a full chapter — Chikitsa Sthana, Chapter 24 — to Madatyaya: the management of intoxication and its consequences. The relevance of this chapter to contemporary male sexual health is not symbolic. It is clinical.
Acharya Charaka wrote in Chikitsa Sthana Ch. 24 on the effect of Madya on Ojas — the vital essence that sustains reproductive and sexual vitality:
“Ojas and its significance has been elaborated here with respect to the liquor effects on the human body; The ojas is the constant energy source of the body which may get affected by the liquor intoxication leading to perplexity which is commonly observed due to liquor.”
Charaka Samhita, Chikitsa Sthana, Chapter 24 — Madatyaya Chikitsa
In the Ayurvedic framework, Ojas is the refined end-product of all seven Dhatus. Shukra Dhatu — the reproductive tissue that governs sexual vitality, sperm quality, and erectile function — depends directly on Ojas integrity. When Madya is consumed chronically, Acharya Charaka describes it as progressively depleting Ojas: clouding perception, weakening Dhatu nourishment, and leaving the body increasingly unable to sustain the physiological requirements of sexual function.
This is not a metaphorical framework. Ojas depletion maps onto what modern endocrinology measures as reduced testosterone, impaired sperm quality, and blunted vascular response. The instrument is different. The clinical observation is the same.
The WHO Global Centre for Traditional Medicine recognises Ayurveda as a traditional medicine system with an evidence base warranting structured evaluation. The WHO Global Centre for Traditional Medicine was established to build this evidence base formally — acknowledging that traditional systems like Ayurveda carry clinical observations accumulated over millennia that deserve rigorous examination rather than dismissal.
What this means practically is that an assessment at Sidri International looks at both dimensions. Dr. Kanu Rajput and Dr. Manu Rajput examine what alcohol has done at the hormonal and vascular level alongside what it has done to your Dosha balance and Dhatu integrity — because these two pictures together give a clearer view of what is recoverable than either alone. View the assessment process and consultation fees
The next section covers exactly how this assessment works and what it examines in men whose sexual health has been affected by regular alcohol consumption.
How Sidri International Assesses Alcohol-Related Sexual Dysfunction
Dr. Manu Rajput, BAMS (known in classical Ayurvedic texts as an Ayurvedic Sexologist and Male Sexual Health Specialist), has over 15 years of clinical experience in male sexual health assessment. The online evaluation is conducted entirely by Dr. Manu Rajput — not a junior, an assistant, or a chatbot. Dr. Kanu Rajput, BAMS, with over 12 years of experience in Ayurvedic formulation, prepares any customised medicines based on the assessment findings.
The assessment process begins with a structured Patient Information Form that captures the full clinical picture before consultation time is used. This includes alcohol consumption history, duration and pattern, current and prior sexual function, hormonal investigation results if any, and the man’s constitutional baseline. This information allows Dr. Manu to move directly into condition-specific clinical questioning during the consultation itself.
Level 2 — Detailed Assessment and Evaluation:
Component | Detail |
Detailed Assessment and Evaluation | INR 5,500 |
Conclusive Consultation | INR 1,500 |
Total Level 2 fee | INR 7,000 |
Follow-up after Level 2 | INR 1,500 per slot |
Level 2 fee charged again for follow-up | No — INR 7,000 is not charged again |
Consultation format | Online — WhatsApp + voice call |
Who conducts assessment | Dr. Manu Rajput directly |
Who prepares formulations | Dr. Kanu Rajput |
The Level 2 consultation fee of INR 7,000 covers the complete two-component process: the Detailed Assessment and Evaluation (INR 5,500) and the Conclusive Consultation (INR 1,500). This INR 7,000 is not charged again for subsequent follow-up consultations. Follow-up slots after Level 2 are charged at INR 1,500 per slot — the same rate as Level 1. Please verify current fees on the pricing page before booking.
For men whose sexual decline appears linked to alcohol use, the assessment specifically examines: the hormonal picture (testosterone baseline, LH/FSH pattern if investigations exist), the vascular and neurological pattern (erection quality, ejaculatory timing, sensation), the psychological layer (presence of performance anxiety cycle), and the Ayurvedic constitutional picture (Dosha dominance, Shukra Dhatu status, Ojas assessment through clinical indicators).
Sidri International’s customised medicines are supplied by courier across India in discreet packaging, typically within 2–3 working days of dispatch. Patients outside India — including NRIs and international patients — are served through online consultation. Medicine availability and courier logistics for international patients are discussed directly with the clinic via WhatsApp.
The next section answers the questions men most commonly ask about alcohol and sexual health before deciding whether to seek a formal assessment.
What Men Ask About Alcohol and Sexual Health
How Much Alcohol Causes Erectile Dysfunction?
There is no universal threshold, because the effect depends on frequency, duration, body weight, and baseline hormonal status. Research consistently shows that sexual dysfunction rates are significantly elevated in men who drink regularly over months and years — not only in men who drink to the point of dependence. If alcohol is a regular feature of your week and your sexual performance has declined, the drinking pattern is a reasonable first variable to examine.
Does Alcohol Permanently Damage Testosterone Levels?
Chronic heavy drinking causes sustained suppression of the HPG axis and Leydig cell function. In most men, this is reversible with sustained abstinence or significant reduction — but recovery is slow, typically measured in months, and depends on the duration and severity of the drinking pattern. Men who have drunk heavily for many years may not fully recover testosterone levels. Early assessment and intervention improves the recovery picture.
Can Stopping Alcohol Reverse Erectile Dysfunction?
In cases where the dysfunction is primarily vascular and hormonal — rather than structural or psychogenic — significant improvement is possible with abstinence. The vascular mechanisms (eNOS recovery, NO restoration) can improve over weeks to months. Testosterone recovery follows a slower timeline. The performance anxiety loop, if it has consolidated, requires separate attention — because it will persist even after the physiological drivers have resolved. Sidri International’s FAQ page covers what to expect from the assessment process.
Can Alcohol Change Your Sexuality Permanently?
Through sustained HPG axis suppression and dopaminergic pathway remodelling, chronic alcohol use can alter the hormonal and neurological substrate of sexual interest and response over time. Whether these changes are permanent depends on the duration, severity, and the man’s constitutional response. Men who address the problem early — before structural tissue changes occur — have the best recovery outcomes.
Does Alcohol Affect Sperm Quality and Fertility?
Yes. Oxidative stress generated by alcohol metabolism damages sperm DNA, reduces motility, and alters morphology. This dimension is often missed on basic semen analysis. For men trying to conceive, the sperm quality picture deserves assessment alongside the erectile and libido picture — they share the same upstream mechanism (oxidative stress and Shukra Dhatu depletion).
What Does an Ayurvedic Assessment Look For in Men Who Drink Regularly?
The Ayurvedic assessment examines which Dosha imbalance is dominant — Vataja (neurological pattern, anxiety, erratic function), Pittaja (inflammatory pattern, burning, hormonal heat), or Kaphaja (sluggishness, low drive, weight-related hormonal suppression). It also assesses Shukra Dhatu status through clinical indicators and examines the Ojas picture. This constitutional map determines what formulation approach Dr. Kanu Rajput designs and what dietary and behavioural framework is most appropriate for that individual’s recovery trajectory.
Pathway B: If the assessment determines that a customised formulation approach is appropriate, Dr. Kanu Rajput prepares medicines in a 10-day supply cycle — typically three sets per month. After each set, the patient shares a structured feedback update, and the formulation is refined accordingly. This is not a generic supplement protocol. It is a medicine cycle designed specifically for your Dosha-Dhatu picture as assessed by Dr. Manu and formulated by Dr. Kanu. WhatsApp Dr. Manu Rajput to begin the assessment process.
[RED FLAG BOX — START]
When to Seek Immediate Medical Attention
The following situations require urgent in-person medical care — not an online consultation:
- Chest pain or pressure during sexual activity or physical exertion
- Priapism: a painful erection lasting more than 4 hours that does not resolve
- Blood in urine or semen that appears suddenly
- Sudden severe pelvic or groin pain
- Signs of acute alcohol poisoning: loss of consciousness, seizure, difficulty breathing, unresponsive state
These are medical emergencies. Go to your nearest emergency facility immediately.
[RED FLAG BOX — END]
CTA CLOSING SECTION
Sexual dysfunction linked to alcohol is not a character failing, a permanent sentence, or something that resolves on its own without understanding what has actually been disrupted. The hormonal, vascular, neurological, and Ayurvedic dimensions each tell part of the story.
Dr. Kanu Rajput and Dr. Manu Rajput at Sidri International Skin Hair & Sexology Clinic assess this picture online — structured, private, and conducted entirely by the doctors themselves. WhatsApp Dr. Manu Rajput to begin.
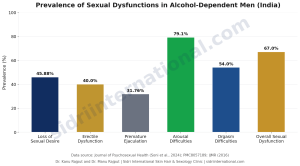
Prevalence of sexual dysfunction types among alcohol-dependent men across Indian clinical studies — compiled by Dr. Kanu Rajput and Dr. Manu Rajput, Sidri International Skin Hair & Sexology Clinic.


